

The Vaccine Question
The Vaccine Question
Given that the Covid vaccines are a dangerous failure, what does that mean for all the other vaccines we inject our kids with?

Thus far, we’ve said a lot about the dangers of the Covid vaccines here.
Despite relative quiet in the past six months, nothing has changed. This means that excess deaths, particularly heart-related, cancers, and other mysterious “sudden deaths” are still at the elevated levels they have been at since April of 2021.
All told, this mysterious cause (consider it to be “Factor \/” as dubbed by the Ethical Skeptic) has killed 600,000 Americans - more than World War I and World War II… combined. This is based on his thorough analysis which I detailed the methodology of the cancer portion of that here:
Cancer's Great Rise - Safe & Effective #14

Now, by latest tallies, only ~17% of Americans received the latest booster, so it appears that most people, slowly, have figured out quietly that these things are no good. That 17% is still far too high, but when you figure 24% of the country still think we are on the “right track” or 16% approve of the job Congress is doing, you realize how hard it is to convince people even if your evidence is rock solid (and you can imagine these three things have pretty high correlation).
Of course, the FDA has just approved the latest Covid booster which, of course hasn’t been through proper clinical trials. And because you are reading this and aren’t a complete idiot, you are not going to listen to them. But it’s important to communicate this as many are susceptible to the effects of sustained society-wide propaganda.
Anyway, let’s move on to more intellectually interesting topics where the case isn’t quite as clear-cut. That is: what about all the other vaccines?
The Childhood Vaccine Schedule
I’ll say upfront: my goal is not to tell any parent what to do or prescribe a specific action at the end of this. I hold parental rights to be a paramount consideration: no one knows what is best for a child better than their own parents.
Along those lines, most sources used here are listed at the bottom of the article. Please take a look, dig in, and ask questions both here and anywhere else!
And, of course, I am not a doctor, and so you should not consider anything said here to be medical advice for you personally.
But what I do hope to do is inform you, the reader, on some historical context and first principles that prompt you to do some thinking and, importantly, ask questions before just accepting the pediatrician’s recommendation.

Here are seven factors that you should be aware of and weigh into your decision making on the subject.
Expansion of the Schedule
Since 1986 (we’ll get to the importance of this date shortly) the vaccine schedule has gone up from 3 series totaling 11 shots to 13 series totaling ~52 shots today.
Prior to 1986, the three series were:
DTP or Tdap (Diptheria, Tetanus, and Pertussis)
Polio
MMR (Measles, Mumps, and Rubella)
Those we’ve all probably heard about to some degree. Since 1986, the following have been added:
1987 - Hib (Haemophilius influenzae Type B)
1994 - Hepatitis B
1996 - Varicella
1998 - Rotavirus
2000 - Hepatitis A
2002 - Influenza
20002 - Pneumoccocal
2006 - Meningoccal (MCV)
2007 - HPV (Human Papilloma Virus)
2022 - The Covid “Vaccine”
International Comparisons
No other country has as many recommended or required vaccines as the US. Of the 13 series mentioned above, here are a few comparisons from European countries:
Sweden: 8 recommended series
Germany, France, and Spain: 11 recommended/required series
Denmark: 6 recommended series
Does that mean one answer is right or wrong? On its face, no. Perhaps 13 vaccinations is best. Perhaps 6 is. But the question is absolutely up for debate! Is Denmark filled with anti-vax nutjobs? Almost certainly not - they’ve come to different conclusions than us presumably through research and it is worth debating which approach is better.
Let’s look at childhood mortality rates in these countries over time. To be sure, this is influenced by a number of factors, but it’s worth noting that the U.S.’s rate has declined much more slowly since the 1970’s than all the rest of these countries:
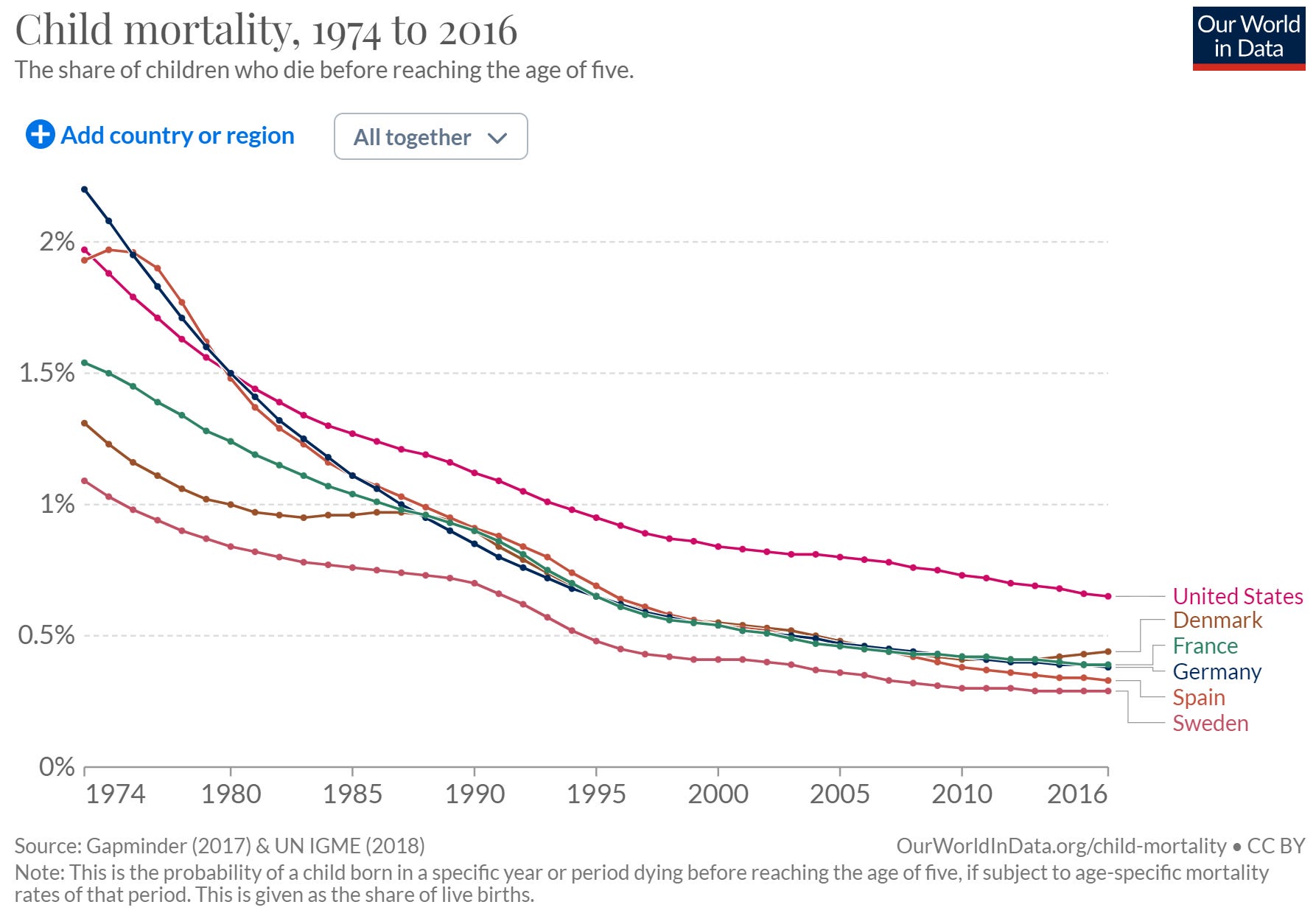
Again - a ton of factors here, so we should not draw from this that vaccines have been a net negative, but being so vax happy obviously hasn’t made our kids any safer. In the 1970’s our childhood mortality rate was similar to Germany and Denmark. Now, their childhood mortality rates are half of ours.
If you are curious, here is the comparison by vaccination series:
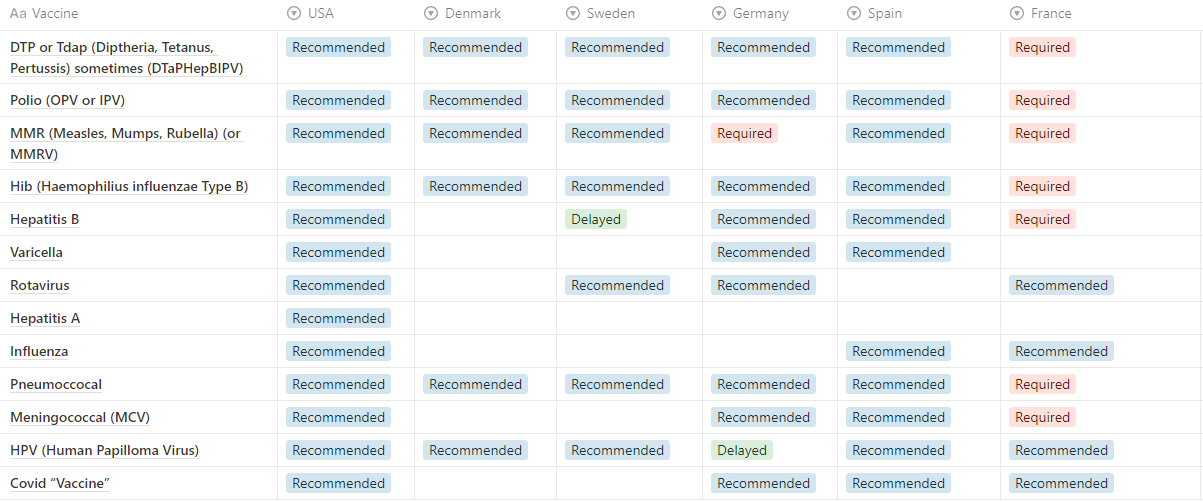
Perhaps a good question for a doc about to give your 2-3 year-old a HepA shot is “This shot is not on the Danish, Swedish, French, German, or Spanish vaccine schedule. And they all have lower childhood mortality than we do here. Why do you think my child needs this?”
Removal of Liability
Let’s return to that 1986 date. It was in 1986 that vaccine manufacturers were given complete (legal) immunity for any side effects or injuries caused by the vaccines.
Now, you can see a logic behind this: vaccines provide a broad public good (if they work) and thus there is a justification to having the costs borne by the public.
But it’s also important to recognize that this comes with several perverse incentives:
Manufacturers only need to meet whatever safety burden regulators set, rather than having negative costs associated with safety issues.
The government thus has an incentive to downplay any safety concerns which would call this arrangement into question and require disbursing more funds to those injured.
Vaccine Economics
One basic economic fact is that any industry will seek profit, likely until the opportunity is gone. Further, it will continue to look for ways to expand that opportunity as long as there is profit to be found.
This is not, by itself, a bad thing. Capitalism works to meet market needs, generally.
However, we have a couple perversions here to a traditional case:
Mandated audience - childhood vaccines are mandated or pseudo-mandated by the government, with marketing done by pediatricians.
No legal cost - as noted, legal immunity removes any substantial legal cost
What we end up with in this case, as with many others is termed an “Industrial Complex” where self-reinforcing mechanisms help an industry build far beyond its natural bounds.
Pharmaceutical companies will keep making vaccines since they are available for a mass audience and incredibly profitable, all the while using lobbyist connections to reduce safety bounds and regulatory hurdles. The government will promote vaccines via the “vaccines = good” messaging that people have accepted and most people will accept without much question.
If these things are bad for you, shouldn’t doctor’s push back? One might ask. Prior to 2021, I’d assume this would be the case as well. Yet we saw doctor’s fail utterly with the Covid “vaccine”. Despite clear and obvious issues, most mindlessly accepted the government line.
In the case of childhood vaccinations, these vaccinations are the primary driver of most pediatrician’s business. The exact numbers are hard to get at and subject to debate, but various incentives are passed via the government through insurance companies to doctors to ensure they have a financial incentive to fully vaccinate your kids. Here’s one example from BlueCross BlueShield that is well worth a read.
The Rise in Systemic Disease
As many know, autism is often the go-to condition most commonly discussed within the vaccine debate. We do know, based on the CDC’s own data, that diagnosed autism rates have risen from 1 in 150 for kids born in 1992 to 1 in 36 for kids born in 2012.
That is a huge (~5x) rise in a relatively short period of time. While some claim that this is just “better diagnosis,” most studies suggest that is, at most, part of the cause not the whole thing.
Given that, what is clear is that something is happening. It could be vaccines, but it could also be processed sugars, pesticides and other chemicals, microplastics, or many other things that have changed substantially since the 1970’s.
But let’s look beyond autism. Various other systemic conditions have seen dramatic rises in the past 40 years.
Autoimmune conditions have seen a 50% rise (from 11% to 16%) since 1988. Severe food allergy rates have doubled or tripled since the late 1990’s. And overall childhood disability rates have increased by 10% from 3.9% to 4.3% from 2008 to 2019. And asthma rates have risen modestly over time.
Now, all this comes as we’ve (broadly) cleaned up the water and the air since the 1970’s. So this is an anathema. We’d assume rates of all these conditions should be going down… unless something else is happening.
Lack of Placebo-based Controls
“Ah, but vaccines have been rigorously tested!” You might say (I would have before 2021). There’s no way that vaccines would cause these signals without us knowing about it!
But alas, there have been some shortcuts taken over time. It’s been a long time since a vaccine was truly tested against a true saline placebo.
Rather HHS (Health and Human Services) has decided that “inert placebo controls are not required to understand the safety profile of a new vaccine, and are thus not required.”
Indeed, when we look at all of the vaccines on the schedule, we’ll see that almost all vaccines now approved were tested against another vaccine as the control group (at best) or no control group (at worst):

Put simply: vaccine science is a house of cards, each additional layer relying on the previous one’s assumptions. This “game” would guarantee that baseline adverse event rates are driven up over time. While any given jump may not be large and could be deemed “statistically insignificant,” the end effect could be quite substantial.
It’s like the game of telephone that you probably played as a kid in schoool: one kid starts the chain with a sentence of “The man jumped over the fence” and by the end of the class people are saying “A merchant sold five cattle.”
Beyond the obvious problem of using other vaccines instead of placebos in individual cases, is that there are not any wholesale analyses of the broader impact of so many vaccines given to kids in early childhood.
One viable hypothesis is that any single vaccine may actually be safe, but the cumulative shock to a kid’s immune system is sufficient to cause some of the issues we mentioned in the previous point.
And that idea isn’t a rabbit being pulled out of a hat: there is a reasonable causal hypothesis as to how this could work.
How Adjuvants Work
The way that most of us were taught that vaccines work is that they expose the body to a little bit of a similar illness (e.g. cowpox was used for the smallpox vaccine), the dead (inactive) particles of the actual virus, or a small amount of live particles of the actual virus.
Long story short: the similar illness approach is not often viable as you need a very similar but less serious disease. So most vaccines (prior to mRNA “vaccines”) are either inactive vaccines (HepA, Flu, Polio, and Rabies) or Live attenuated viruses (MMR, Rotavirus, Varicella). Lastly, others user a specific part of the virus rather than the whole bit. These are recombinant vaccines and are used for Hib, HepB, HPV, Pneumococcal, and Meningococcal.
With the exception of the live attenuated vaccines, the problem is that the body isn’t going to view dead or inactive particles or parts of particles as a threat, so the default immune response would be to do almost nothing and thus have no short-term or long-term benefit.
To get around this, inactive and recombinant vaccines use adjuvants: toxic chemicals that our bodies will react to. Our immune system then associates the inactive viral particles with the toxicity of the adjuvants and boom, you have an immune reaction!
So this does work: i.e. it is an effective way to get a human to have an immune response to a given particle.
Safety, however, is another question. A common adjuvant used in current vaccines is Aluminum, which is toxic to consume and in addition to acting on the viral particles may create allergic reactions to many other organic and inorganic chemicals that the body is exposed to around the time of vaccination, including things within the person’s own body (i.e. autoimmune conditions). And back to the point on the lack of studies: maybe one dose with aluminum is okay, but what about 50 doses?
The CDC acknowledges that they use adjuvants but claims that these are safe. Which, again, may have carried some weight 5 years ago but is not good enough today.
Conclusion
As I said upfront: I’m not going to prescribe action here. But you can consider several options:
Go Conventional - Ignore all this and just take all the shots that your pediatrician recommends.
Slow down the schedule - many parents have worked to delay shots in an effort to spread out the total shock to a child’s body and immune system. Under the theory that the negative effects are cumulative rather than due to any one shot, this has solid reasoning for reducing the risk of negative side effects.
Pick and choose - the fact is, not all diseases (and not all vaccines) are created equal. Many of the newer vaccines treat diseases that, yes, could be serious, but only in incredibly rare cases. You can make a case-by-case decision on each vaccination.
For example, let’s take MMR (Measles Mumps Rubella) - this one has been around for a while, uses a live virus approach, has no adjuvants, and is given broadly in Europe as well. This is likely a better bet than HepA (newer, not given anywhere else, has aluminum adjuvants).Go back to 1986 - vaccines introduced prior to 1986 were made back when companies could actually be held liable for negative impacts. Thus, an incentive-based analysis would lead you to assume that these are safer options. By going back to the 1986 schedule, you’d also greatly reduce the cumulative vaccination load.
Go No Vax - this is an option too. And frankly, it’s one I considered crazy… until 2021. Now? Well, let’s just say I view it a lot differently, and one worth further investigation.
As Jonah Goldberg wrote, back when he was smart, modern Americans have a strong tendency and desire to outsource our critical thinking to others. This is an exceedingly bad trait and one I’m not going to let you indulge in. As a parent reading this, this is your choice to make.
Sources
European Vaccine Schedules: https://www.ecdc.europa.eu/en/immunisation-vaccines/EU-vaccination-schedules
US Vaccine Schedule: https://en.wikipedia.org/wiki/Vaccination_schedule
Childhood Mortality Rates: https://ourworldindata.org/child-mortality
CDC Autism Data: https://www.cdc.gov/ncbddd/autism/data.html
Autoimmune rates over time: https://www.everydayhealth.com/autoimmune-diseases/autoimmunity-rates-on-the-rise-in-the-united-states-study-says/
Allergy rates over time: https://www.lucieslist.com/guides/starting-solids/early-introduction-of-allergens/
Childhood disability rates over time: https://www.census.gov/library/publications/2021/acs/acsbr-006.html
Asthma rates over time: https://www.cdc.gov/vitalsigns/asthma/
HHS on placebo controls: https://childrenshealthdefense.org/wp-content/uploads/hhs-response-january-29-2018.pdf
CDC Adjuvants used: https://www.cdc.gov/vaccinesafety/concerns/adjuvants.html