


Vacc-sanity
The Covid Vaccines were supposed to make the situation better. But they haven't. Let's figure out why.

If you haven’t yet read last week’s piece, The Two Covids, please check that one out first.
Now, let’s talk about the vaccines. This will be a long one, but I want to build the case I’m presenting here in one uninterrupted piece.
If there is one lesson that pharma companies will take from the Covid Era, it is this: just call your product a vaccine. Even if it isn't. Just do it and watch the wagons circle and the profits come chugging in.
So let's start off with some of these hard, controversial-but-true statements. The Pfizer, Moderna, and J&J Covid-19 products are NOT vaccines by any conventional understanding of the term. Prior to 2020, a vaccine was a substance that "stimulates a person's immune system to produce immunity to a specific disease."
But as even the CDC knows: these products don’t fit that definition. What’s a friendly government agency to do?
That should be obvious: change the definition of vaccine. Problem solved! Yes, in case my sarcasm is confusing you: the CDC quite literally changed the definition of what a vaccine is so that the Covid products would qualify.

Call me old fashioned, but I believe words have meanings irrespective of the whims of a governmental agency. These products don’t meet the definition of a vaccine. As such, they will be referred to throughout the rest of this piece as therapeutics.
And there shouldn’t be anything wrong with that. The products can be defended as therapeutics, certainly for those who are at high risk!
If all this already sounds like we’re living in some kind of Alice in Wonderland type scenario… get used to it, because there is a lot more where that came from. When you look at how the therapeutics have been handled in the past year, there’s a lot more of that.
A Quick Macro Perspective
We could spend hours going through things country by country, debating seasonality vs. variant waves vs. the impact of therapeutics or other attempted interventions. But holistically it comes down to this:
Many countries have now reached 70-80% adult vaccination rates (or higher) and are still seeing high degrees of viral spread, excess death, and thus are bringing back NPIs (Non-Pharmaceutical Interventions) like masks, social distancing, and even lockdowns.
Here in the U.S., we have gone from having 0% of adults vaccinated at the start of 2020 to almost 80% of adults vaccinated by November. Despite that, we are on track to have more excess deaths this year than we did last year.
No matter how much you want the “vaccines” to have worked and bring back normality, any intellectually honest look at this has to question just what the heck is going on. Because it is pretty damn clear that these products won’t end Covid. Once we actually look at the evidence, it’s pretty easy to understand why. Let’s dive in.
Therapeutic Efficacy
Putting the “f” in Efficacy… twice I guess.
The products that we have at our disposal (and you could include AstraZeneca and the Chinese and Russian products) are not producing immunity. Their response is, at best, short-lived to a ~6 month period before they, at best, become ineffective.
A recent paper in Science highlights just how ineffective vaccines become over the first 6 months. Here is the graphical summary of their work:
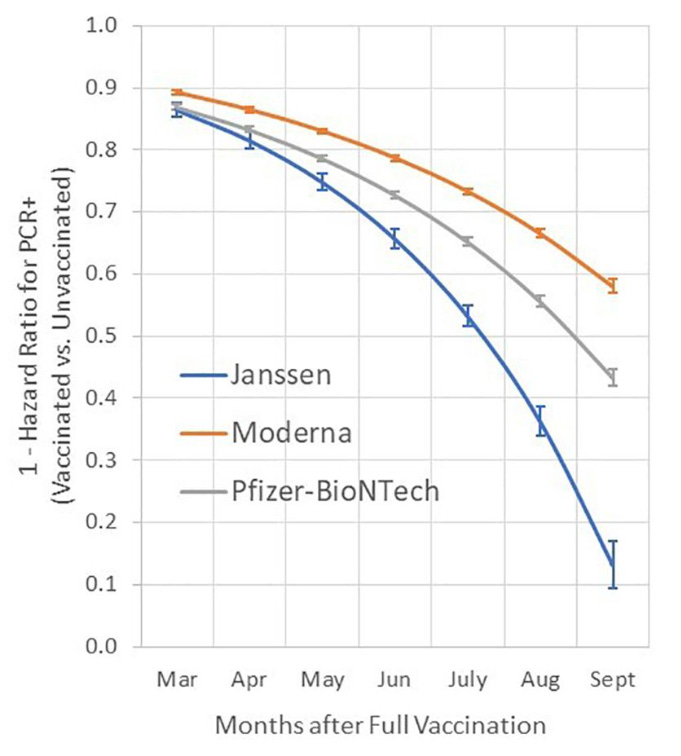
Here’s a quick interpretation of it: after 7 months (the cohort analyzed was jabbed in February) in September, the J&J vaccine is ~15% protective against infection, the Pfizer is ~42% effective, and the Moderna is ~58% effective.
Just as importantly: these trends are accelerating toward zero rather than leveling off. If you see enough data like this, you know that these trends will end at 0% efficacy. J&J looks like it’ll hit it by month 8, Pfizer is probably around month 11, and Moderna probably around month 12.
You may not like to hear this, but the data doesn’t lie. And once again, this was so clear based on the experiences of Israel and the UK that a brilliant idea was born: booster shots!
Let’s Get Boosted?
The definition of insanity is doing the same thing over and over again and expecting a different result.
When your therapeutics stop working, what are you to do? Jab it again!
Okay, sorry for the snark - let’s take a look at the evidence for booster shots. We’ll again go straight to the CDC for this. What do we find? Well, the clinical trial for the 3rd Pfizer shot only included 306 participants in its safety analysis. This isn’t nearly enough to do much of anything frankly. Basically they checked to see if antibody counts increased and then checked for any side effects in an underpowered sample.
Critically, there is no evidence from this trial about long-term efficacy (or safety). There quite literally can’t be any because there hasn’t even been enough time passed to see if the decay curve from the third jab follows the data from the second jab that we see up above.
Israeli analysis is suggesting that the Pfizer booster should offer protection for 9-10 months, but that should be read as being basically in line with the second shot. But at the same time, they are also preparing citizens to get a fourth shot if they want to keep their freedoms.
Long story short: these boosters follow a similar (read: declining) efficacy curve. The people in charge know it, but they have no incentive to let you know.
Pandemic of the… Vaccinated?
Despite the CDC’s propaganda, data from the U.K. shows that the vaccinated are much less safe than presumed.
While the U.S.’s tracking and analysis mechanisms have failed to gather accurate data, we do have fairly robust data from the U.K.
In the U.K., about 80% of the hospitalizations and deaths are among the vaccinated in recent months. See data from the U.K. here through September.
Now, that does not mean that the therapeutics are ineffective. Indeed, when you look at the stratification by age, you’ll see a ~70-80% reduction in death rates within an age group. But because Covid deaths are so stratified by age, and because most older people have received the therapeutic, most of the burden on hospitals is still the elderly.
The same data set also presents some interesting findings with regard to relative frequency of Covid infections. Recent data suggests that adults who have received the therapeutic have higher rates of Covid infection than those who have not. While the evidence may not be strong enough to suggest that the therapeutic enables infection, it should put the nail in the coffin of the idea that these products are at all protective against infection. That is clearly not the case:

Can’t Stop, Won’t Stop (That Transmission)
It gets dumber. It always does.
So as we’ve established, these vaccines become ineffective relatively quickly with regard to preventing infection. So let’s now take a step back and look at what that means for the transmission, or spread, of the virus.
It should be obvious then that the vaccine won’t stop the spread of the virus. Because if you are infected, then you can transmit it, and this virus transmits quite easily. Even if we give you the best case scenario where we jab everyone every six months (sounds fun, right), you are still hitting ~60% efficacy by the end of that period. The virus will still find a way to circulate, especially if the estimates of the Delta Variant’s transmissibility are accurate.
This reality is further bolstered by a study from UC Davis study that found no difference between the viral loads of vaccinated and unvaccinated people who were infected with Delta.
This shouldn’t come as a surprise for anyone: it’s been known for some time that these therapeutics are non-sterilizing, or “leaky” for short. This essentially means that the therapeutics mask the symptoms, but don’t actually stop the virus from replicating inside of you.
This creates several problems. But when it comes to transmission the problem should be quite clear: vaccinated individuals are more likely to have their symptoms masked by the therapeutic and thus much more likely to be going about and transmitting it than someone who presumably has symptoms and tries to stay away from others.
One last thing on this: all of these insights are further validated by macro data at a state or country level. Many countries saw steep rises as they began their vaccination campaigns. This is confounded by the Delta Variant to some degree. But we even see in small countries/regions like Gibraltar, Singapore, and Iceland where despite close to 100% vaccination the virus is still spreading steadily.

If the vaccines don’t work in small countries (that can apply strict immigration controls) with 90%+ of adults receiving the treatment, then they sure as heck aren’t going to work in bigger and looser countries like the U.S.
Leaky Drug During a Pandemic… What Could Go Wrong??
A lot, potentially.
Diseases like Polio and Smallpox were eliminated because the vaccines produced for them were sterilizing. This means that the vaccine trained the body to fight the pathogen and prevented the pathogen from ever replicating to a large enough scale where it could be passed from person to person.
As we have established, these therapeutics do not do that. The virus still gets in, can replicate to levels similar to someone without the shots, and still be transmitted similarly as well.
One of the voices that is talking about the potential issues we’ll run into is Geert Vanden Bossche. You can check out a comprehensive interview with him here.
The gist of it is this though: because the virus had already started to mutate and is broadly present worldwide, leaky therapeutics will help to train the virus and make it more likely that a strain emerges that is able to circumvent the therapeutics. Because transmission is on-going even among those who have the jab, the virus is getting, quite literally, millions of at bats to test out slight variations and see which ones are more effective at taking hold in an admittedly tougher environment (therapeutic present). Just like a baseball player that gets trained by trying to hit the pitches from adults, the player that emerges from that training successfully will become dominant.
This may sound like anthropomorphizing, but evolutionary tactics work in this way. Beneficial adaptations (from the perspective of the virus) will be more likely to dominate, grow, and spread. This is how humans evolved and how all life forms have found their niche. Viruses trained in “tougher” environments will become the fittest.
What is the end result? Geert and others suggest that the arrival of a fully-resistant strain of Covid is almost a certainty. What do we do then? Do we try to play the same game again? We would only find ourselves in the same spot a year or two down the road as the virus would inevitably mutate again to evade the next version of the therapeutics.
Safety First… Except This Time!
Safety-ism plus mass psychosis leads to some interesting results.
Here is an inconvenient fact: these therapeutics are some of the most dangerous treatments out there. They have killed tens of thousands and injured millions worldwide.
This may surprise you. It may trigger you. Or it may make you breathe a sigh of relief that someone is finally saying what we all know. We’re going to start with the evidence, and then jump to why this information is being systematically censored.
Regardless of how you feel, the facts don’t care. There have been at least 8,000 deaths, permanently disabled 10,000 more and led to 40,000 hospitalizations in the U.S. submitted to VAERS. This dwarfs the number of reports in previous years:

However, these numbers is just the tip of the iceberg. Because of the incentives in place, most issues with the therapeutics are not being reported to VAERS. There are many testimonials from people with severe adverse reactions whose data was never entered in VAERS. This happens systematically because VAERS reports are time consuming for medical professionals and come with no real incentive to provide. They also need a lot of detailed information that isn’t easily available.
That said, we don’t have a great mechanism for measuring vaccine-related deaths and injuries for the simple reason that it is very hard to prove causality. If you inject a million people in a day, odds are good that some small subset of that million will drop dead the next day due to random chance.
So let’s talk about three ways that we can approximately resolve this issue, and where the data points.
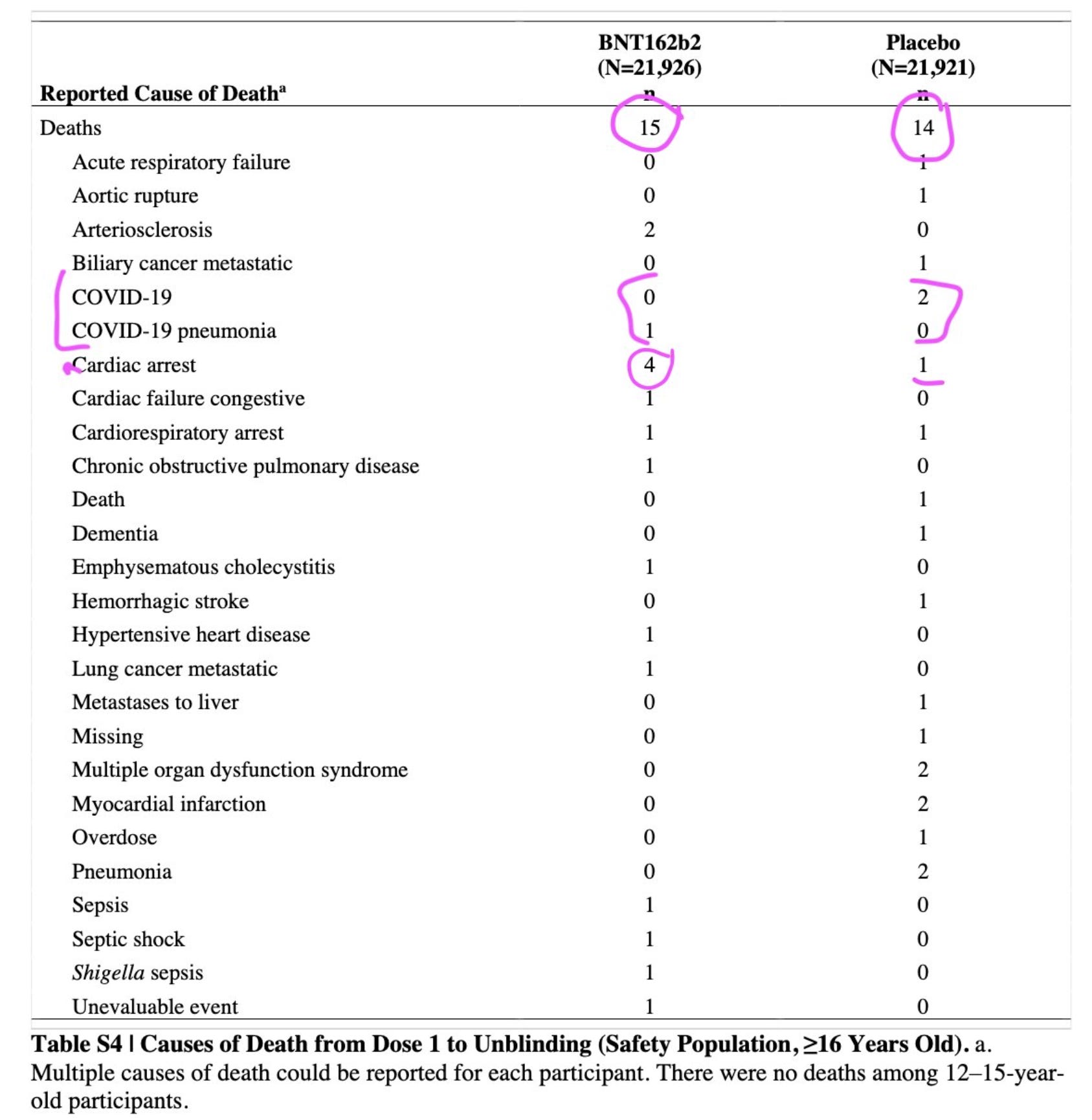
Randomized Control Trials (RCTs) - normally the best approach for any kind of medicine or treatment. All of the therapeutics we’re covering here went through these trials, so we do have data on it. What you might recall from these trials is the excitement over the “95% efficacy at preventing illness.” But what wasn’t covered is as important, if not moreso: none of the products led to a reduction in overall mortality. In Pfizer’s trial there were 15 deaths from those who received the product, 14 deaths in the control group. In Moderna’s trial there were 16 deaths from those who received the product, and 16 in the control group. And the data is currently unavailable for J&J.
The data from the Pfizer trial is particularly noteworthy, as there are 4 deaths due to cardiac arrests in the treatment group - noteworthy given what we know about the impacts of Pfizer and Moderna on the heart:
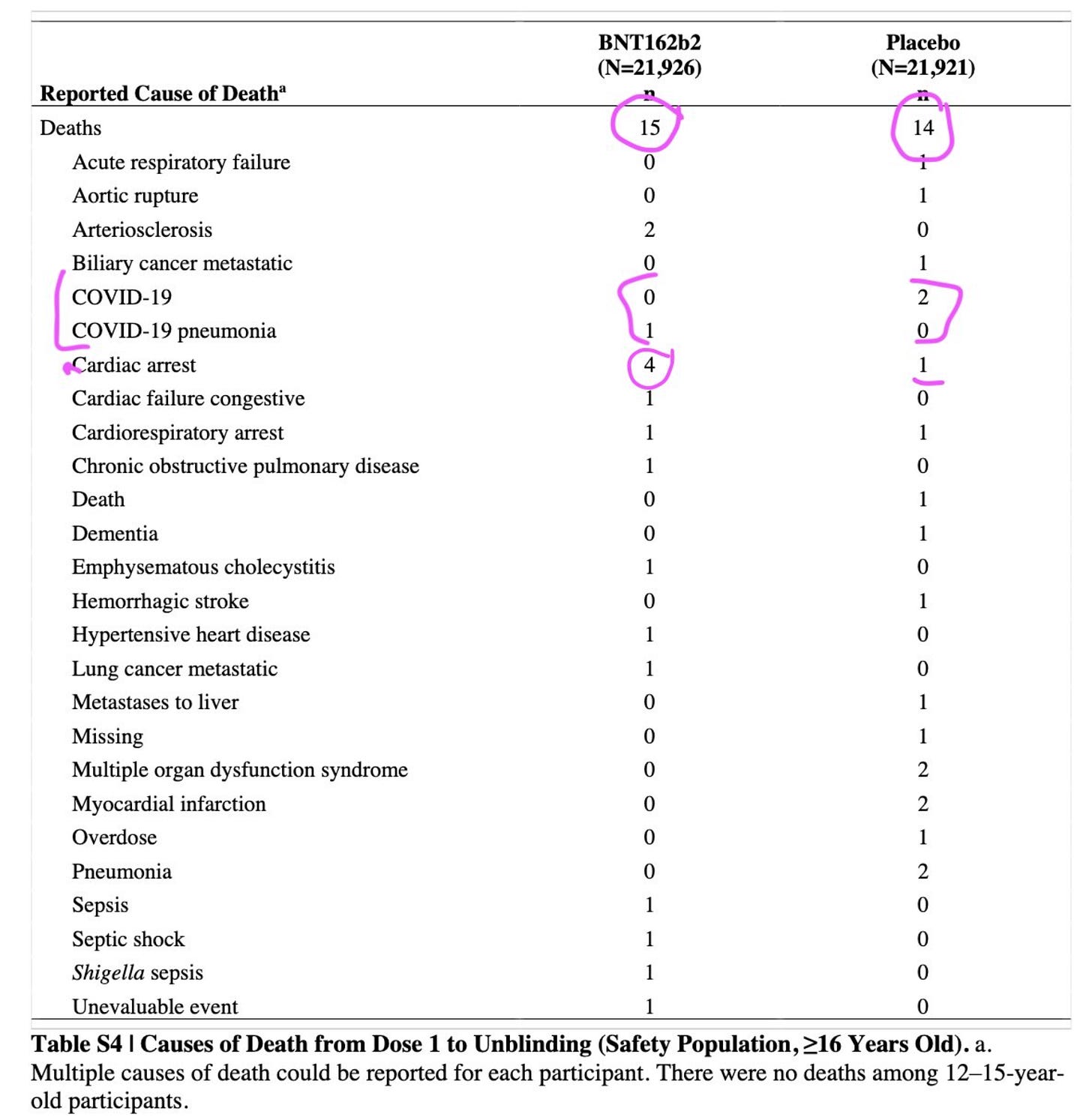
Source: Pfizer And actually, it has recently been discovered that Pfizer may have, uh, miscounted the deaths in the original report, as a recent update now states that 21 test patients died relative to only 17 control patients. While that may not quite be statistically significant (74% significance), it’s not what you’d want from a treatment you plan to give out to hundreds of millions of people.
Time-based comparison - one other option that we can use is to assess mortality during 2021 vs. prior years to see how much more death we are seeing relative to normal. For things like the pandemics (or broad scale rollouts of treatments) this tends to be the best approach. What we see should surprise people: we are on track to have more excess death in 2021 than we did in 2020.
This is concerning because we had basically zero “vaccination” in 2020 and now we’ve had close to 80% of adults “vaccinated.” No matter how you slice it, something is amiss that needs explained. If you go from 0% to 80% “vaccinated” and you have more death at the end of that journey than when you began, you need to start asking some hard questions.
Now obviously some can bring up the Delta Variant as a contributor to this, but that is not sufficient to explain how deaths have gone up.Lastly, you could design a study to look at mortality for people who have had the vaccine and compare it against people who haven’t yet at this point. This is what we would call a “natural experiment.” The challenge with this however is that because there is going to be an inherent bias in who takes part in the experiment, it can be very challenging to measure accurately.
And indeed, that seems to be what happened with a study that did attempt to look at this. The study looks at over 3 million people, and finds that the vaccine reduces non-Covid fatalities by up to 70%. If that sounds unbelievable, well, it is… not believable. For one, an effect that large, if real, would have shown up in the clinical trials. It is an absurd conclusion and it is incredible that something that wrong could be published, let alone by the CDC. Taking even a cursory look at the paper, it is clear that they did not control for income/socioeconomic status nor pre-existing health conditions. The result here is simply displaying a bias in the design rather than any meaningful insight about the safety of the therapeutics.
So where are we at here? Therapeutic safety is a topic we could write about for ten articles and still not convey the full degree of nuance. But the point is this: these products are not some risk-free solution, and should not be treated as such.
For each person, there is a risk from Covid and there is a risk from the therapeutic you take. These risks are different for every person based primarily on their age, health, and whether or not they have already had Covid. If you are 80 and unhealthy, the risk of Covid is likely higher than the risk of the vaccine. If you are 30 and healthy, or certainly if you are a kid, it is the reverse.
A Quick Assessment of Treatment Risk vs. Covid Risk
A practical example of low-probability risk assessment.
Okay, so now we’re going to get into the calculation of this a bit. Let’s take the VAERS data at its word and assume no undercounting is happening (even though we know this is false).
We have 8,456 deaths and 9,770 people who have been permanently disabled. And meanwhile you have administered 434 million shots of the various therapeutics according to the CDC.
This is a low-end estimate of therapeutic risk. There have been almost 10x hospitalizations recorded and many other side effects that, hey, don’t kill you, but do have serious negative impacts. There are a host of cardiac and neurological effects that are plausibly caused by the therapeutic and may not disable you but could make life quite unpleasant.
What does this mean? Doing some basic math, this suggests that there is a 0.0042% chance of death or disablement after one of these shots. Assuming you need two shots, your odds are doubled. So for most people, the odds of death or disablement from the two-shot series is 0.0084% which is about 1 in every 11,900 people.
Is that risky? Humans are not great at understanding very big or very small numbers. That feels safe, right?
The thing is… Covid is also super low risk for the vast majority of people. Fortunately this data is available too! Based on this assessment from Stockholm University, the odds of an otherwise healthy 30-something male without any high risk conditions dying is roughly 1 in 71,000 or 0.0014%.
So what does that mean? For someone like myself, a two-shot regiment of these therapeutics increases my risk of death or disablement by 6 times! And this is best case. Would I need to add a booster? The risk is now 9x. Is VAERS only representing half of the total cases? The risk is now 12x or 18x if I’d need a booster.

And hey, if these products were actual vaccines and actually 100% effective… then maybe that’s a risk I could swallow. Or maybe if it stopped transmission. But based on all available data, they don’t stop transmission and as soon as I go 9-10 months without another shot, I’m going to be right back facing that ‘roni risk. And all that is assuming that the virus doesn’t mutate, in which case all bets are off.
Now at the same time… say I’m a 70-something female still without pre-existing conditions. Now the math changes. My Covid risk is 0.175% based off the same study, so the 2-shot therapeutic is 20 times safer than facing Covid. Now, the risk calculation is not complete in this case since, as we covered, the therapeutic does not fully eliminate the risk of death from Covid. But it is reasonable and still tolerant to a booster or some undercounting.
But for me, and other young and healthy people, it presents an absurd proposition. And kids? Don’t even get me started! By the same source, the Covid therapeutics are 210 times more dangerous for children than Covid itself. The fact that we are giving kids this stuff is flat-out insane. Hopefully the half dose and the blood thinners added to the formulation help make it slightly less dangerous for kids, but it is still an insane proposition and risk for someone to take with their kids.
If we jump to a more sane country, Taiwan has paused the second dose for kids 12-17 due to the substantial risks to the heart, and is not approving any doses for kids under 11. Of course, Pfizer has less lobbyists per capita in Taiwan than they do in the U.S., so perhaps this makes sense.
Oh by the way, this analysis doesn’t even take into account that there are both existing treatments as well as new therapeutics from Merck and now Pfizer purported to provide a 50-90% reduction in Covid risk when taken as an early treatment. This would reduce the Covid risk by 2-10x and thus make the “vaccines” even more risky on a relative basis.
I really can’t understate this: given what we know now, I’d have to be a fucking idiot to get a first, second, or third jab of this stuff.
It doesn’t work, so let’s mandate it?
Mass psychosis gets “legal” backing…
If people were looking at this rationally, then we’d see the following facts:
These therapeutics wear off after about six months.
Even then, they are leaky throughout and still allow the virus to infect and transmit.
Because those who have received the therapeutic can still transmit the virus, there would be no restrictions on movement subject to medical status.
From a macro level, we’ve seen no declines in infection or in excess death this year, despite going from 0% to 80% of adults who have received the treatment.
There are real and serious side effects from the treatment that make it a poor health decision for people who are young and healthy.
For those who are older and unhealthy, the risk from Covid is much larger and likely justifies the therapeutic risk.
As such, the therapeutics should be made available, but only encouraged for those who are at a substantial risk from Covid.
But what do we get instead? We get one-size-fits-all government policy and highly illegal and immoral mandates from companies and the government alike. You should be able to tell by now how objectively stupid such actions are, based on the available data. And as crazy as it has been in the U.S., the policies in almost every other Western nation (bar Sweden) is even worse!
If we are to ever recover our trust in public health and in certain branches of government, then we will need tribunals and the people who have abused their trust and the authority granted to them by the people will need to be held accountable.
Censorship Keeps You in the Dark
How is it possible that much of this information has been kept from the broader public?
The topic of censorship and narrative control could be an essay, or even a book, all on its own.
The quick version is this: it doesn’t take a grand cabal or conspiracy involving a shady group of men sitting in a smoke-filled room. Censorship and cover-ups are often emergent, meaning that they arise naturally based on the situations and incentives that present themselves.
In our case: Covid appeared and was deemed a threat. As these therapeutics were being created, everyone’s interests were aligned toward having them succeed:
Pfizer, Moderna, and J&J stood to make billions
The government stood to be seen as a savior
The media could use them to foment division and improve their click rates
The people would have a way back to normality
Thus, it is understandable that the drug companies may have gamed the clinical trials. And why the government would look the other way then promote the products as safe and effective. And why the media would cover for them to make the new administration look good, and paint any criticism as crazy conspiracy theories. And the general public, weary of the Covid years, would broadly be accepting of the propaganda.
Once the narrative is set… good luck going against it. Bureaucrats in all types of organizations fall into line, and speaking out quickly makes you seen as an outsider. Cowardice keeps most people in line, even preventing them from asking questions.
But a good number are still speaking out. Senator Ron Johnson hosted an expert panel with many of them… which was ignored entirely by the mainstream media, and then the video of the event was censored by YouTube (you can watch it here instead).
There is very little for one to gain by speaking out against this flawed narrative around these therapeutics, but much to lose. On a personal level, I know I risk relationships with friends and family members by bringing this up. This is doubly true for doctors, who in many cases are facing substantial risks to their career and income as well if they deviate from the approved narrative. But trust me when I say that I am speaking for many others who are speaking under pseudonyms or not speaking at all.
A Conclusion
As we covered last week, we sadly live in anything but rational times. The entire “vaccine” saga bolsters the case that we are living through a mass psychotic event. There is so much social pressure to conform. To “vaccinate” yourself and even your kids. And of course, to post selfies about it. To exclude people, to fire them, on the basis of personal medical decisions.
Burn the witch! And don’t you dare ask why, for fear that you may be the next one to be accused of witchcraft. Different centuries, same game.
Stop the madness.
I’ll leave you with one anecdote to personify the data presented above. While I could choose a more sympathetic character (such as the story of Ernesto Ramirez), let’s take a look at the story of a 52-year-old cardiologist, Dr. Sohrab Lutchmedial, in three parts:

I want to extend my sympathies to Sohrab’s family and friends. I hope that his post in July didn’t truly reflect his views, and I am sure that in many ways he was a nice person just trying to help others. I’m sure he helped save many lives during his time as a cardiologist.
But Sohrab’s story should be a warning: one can be smart and qualified, yet still be hopelessly deluded about reality. And the world has a way of eating up those who see the world they want rather than the world that is. Don’t let that be you.
Enjoyed this article? Help me get the word out! Share it, subscribe, and/or leave your thoughts in a comment.
Great article! For those of us who've been following this for the last year or two reading published scientific papers and digging into the data none of this is new. However, this article does a great job of consolidating and summarizing that information, while still remaining relatively accessible. It's hard enough to try and talk to people who are swallowing the main stream narrative on this, when you then follow up by sending a myriad of articles and published papers you read over the last year, that tends to finally shut the awakening down. It seems people would rather trust the main stream "authorities" than read the actual scientific findings or look at the data which thanks to the internet are freely and widely available. Anyway, thanks to this article i now have a manageable resource i can send to people who are starting to wake-up and question what's happening without drowning.
I'm particularly glad you took the time to touch on relative risk. This is the main reasoning where anyone following the main stream narrative seems to have failed but was always my rationale for not getting it. While i am likely labelled as an "anti-vaxxer" my argument from the beginning has never been to not take the vaccine, it's always been that you should look at your risk profile and use that as the basis for your decision. In my case, and for most people under 60 with no underlying health issues, the risk profiles showed it made no sense to get the vaccine.
Anyway, great article if it manages to open at least one more persons eyes to what is happening it will be a solid service to humanity.
This article is everything!! As a fellow healthy 30 something it sums up exactly why I have remained unvaccinated and will now bow to the pressure. Thank you for your detailed analysis and reasoning