


Safe & Effective #6: Covidian Groundhog's Day
The vaccine leads to endless Covid reinfections

Where are we at so far? We’ve seen a 25% increase in emergency cardiac events that happened to start as the vaccines came out:

And we’re seeing an alarming, anomalous rise in cancer deaths that also happened to start right when the vaccines came out:
Then we got distracted by the 3 million newly disabled Americans that also started right when the vaccines came out, a disgraceful presentation of “science” in justifying the jabs for young kids, and the news that the Covid vaccine causes a 15%+ drop in sperm count.
One might say, we’re at this point:

But for those who know the meme, we know there’s a fourth member to this party. Let’s put a name to that guy:

Yes, today we get to wade into the fun world of how viruses evolve and explain why we are increasingly seeing stories like this one:

This is captured in Igor Chudov’s post on the topic of Covid reinfections, and this has even made its way into mainstream media with Bloomberg noting that “others are catching Covid for a second, third or even fourth time.”

As we’ve largely addressed the “Safe” part of “Safe and Effective”, let’s put on our smart hats and wonder how something can be deemed “effective” if you can get jabbed 3 times in a year and you still get Covid 3 times in that year.
Now, Lizzie here illustrates the conventional belief that the vaccines prevent infection. Because, well, that is what real vaccines do. But as we’ve covered, these products are not vaccines and we had to change the definition of vaccine in order to label it as one:
What is actually happening here with the Pfizer and Moderna products is that these products primed the immune system to react in a very specific way. What we call Covid has branched far far beyond the original Wuhan-style O.G. virus that was used as the basis for the “vaccines”. As a result, the body is trained to respond overly specifically. It learns the “Wuhan trick” which works fine enough when you only need the Wuhan trick. But it may or may not work well once you need a second or third trick. Broadly, this is called OAS or Original Antigenic Sin. More colloquially you could consider it the One Trick Pony Syndrome.
An Aside: A Machine Learning Analog
This concept of OAS is seen in many other complex systems. Any data scientist reading this will immediately see the parallels to one of the largest problems they face: overfit.
Let’s say that you want to build a model to be able to read and transcribe handwriting. To do that, you need a training data set and for ease you just use all of your own handwritten notes and no one else’s. What happens?
Well, that model may be great at reading your handwriting, but it’s likely that your model will quickly become useless when trying to read anyone else’s. We taught our model one trick, which is great when that’s the trick you need, but pretty useless in any other scenario. It is overfit to one way of writing, but was trained with no regard for any other ways of writing.
With all that introduction out of the way, let’s substantiate this. Sadly, we see evidence of OAS on two fronts: micro-level antibody analysis and macro-level infection trends.
Micro-Level: Antibody Analysis
Looking at antibody levels in individuals gives us more insight into how and why the immune system would respond like this. I’d highly recommend checking out The Bad Cat’s post on this subject back in October of 2021:

Materially, the evidence for this piece comes from the UK Government’s weekly Covid report, which noted that “recent observations from UK Health Security Agency (UKHSA) surveillance data that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.”
This is corroborated by a study done in the UK that shows unvaccinated individuals have materially higher N-antibody levels after recovery than vaccinated individuals. Further, they see that those with two doses have lower levels than those with a single dose:
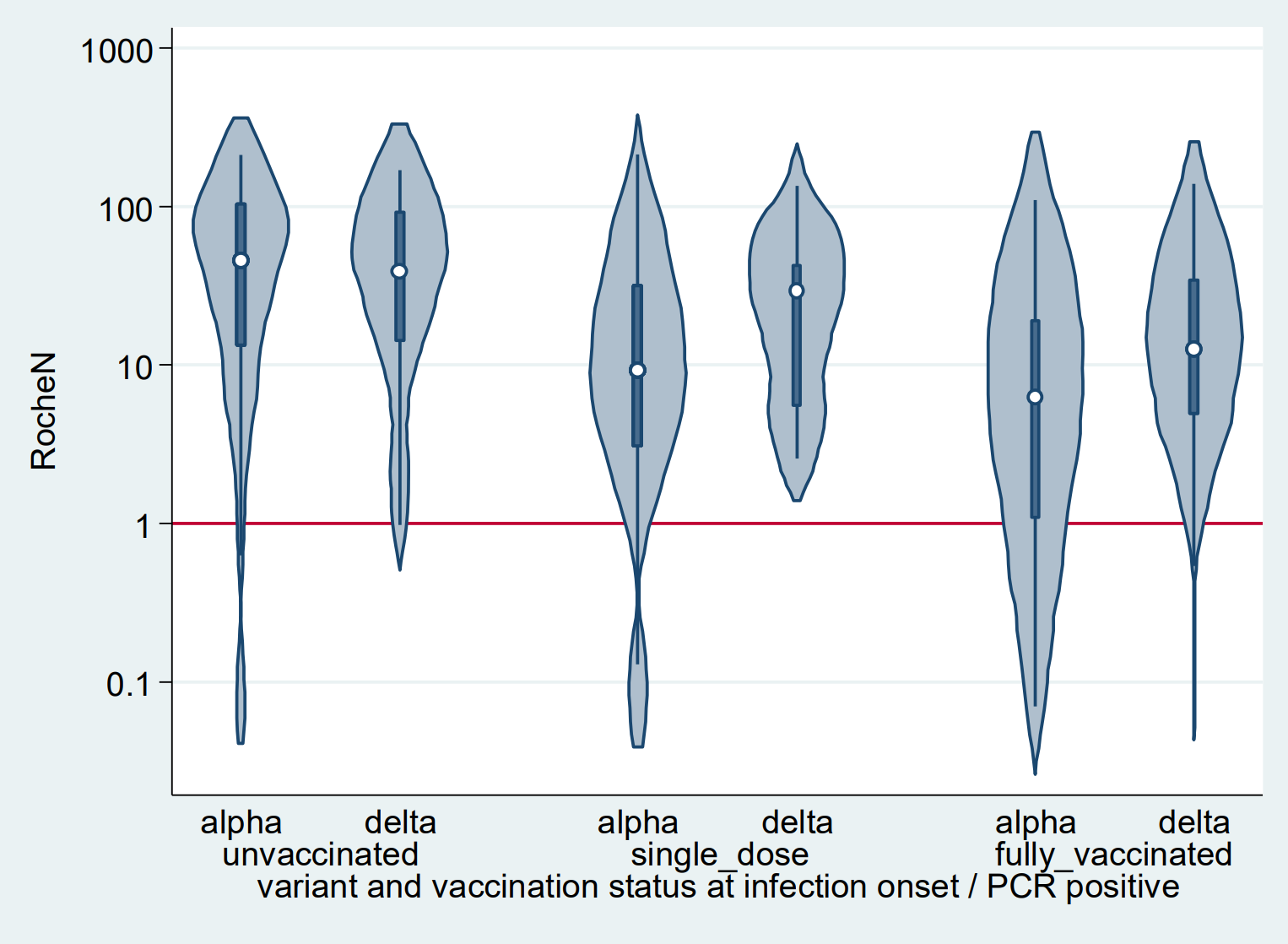
Why does that matter? This quickly gets into a much deeper look at how the immune system works. But what you need to know is that the vaccine was focused on the Spike (S) protein and thus trains the body to produce S antibodies. This, as is now well known, attempts to fight the symptoms of Covid, but doesn’t actually prevent infection.
Meanwhile N antibodies attack the Nucleocapsid protein, which is essentially what houses the RNA of the virus itself. Thus, these do actually work to destroy the virus once it enters the body and starts replicating. As a result, they can work faster and are more likely to provide robust and longer-term immunity if you have them in your system.
Macro-Level: Infection Trends
Aside from our girl Lizzie that we kicked this off with, let’s step back and look at broader trends. We obviously know that vaccinating ~70% of the country hasn’t led to a reduction in Covid cases. Here’s the data straight from the CDC:
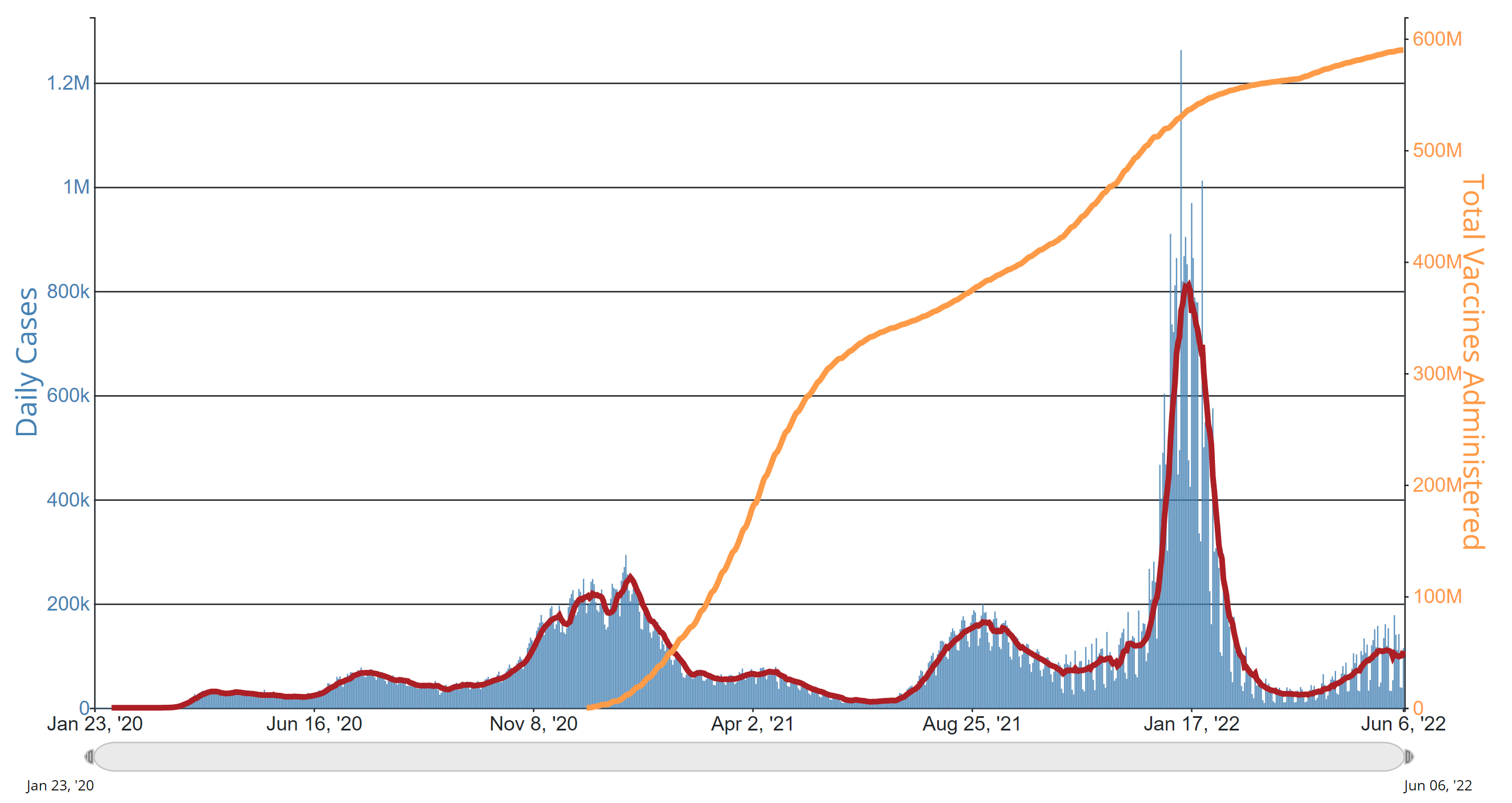
So, the idea that the vaccinations stopped infections is pretty clearly false.
A critique of this simple analysis would be “well, Delta came along, and then Omicron.”
The answer to that critique is “Exactly.” The variants that rose to prominence did so precisely because they had the capability to escape the “vaccine.” Vaccine-evasive variants were essentially guaranteed the minute we started mass vaccination (rather than targeted vaccination) mid-pandemic with a leaky (non-sterilizing) vaccine.
This can be misinterpreted, so I’ll clarify a bit. Viral evolution is natural: you are going to have hundreds of slightly different permutations of the virus out there in the world at any given time. Actually tracking these evolutions looks something like this:
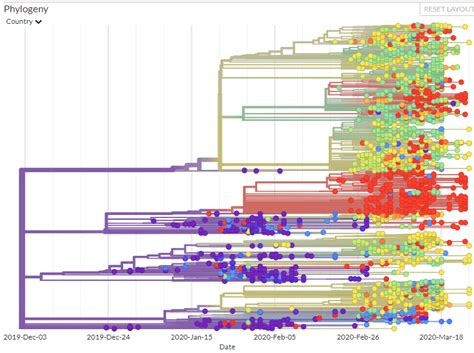
Most of these evolutions are functionally equivalent, and most go nowhere. But what happens when you introduce an evolutionary pressure like a vaccine? All of a sudden, those that are impacted by the vaccine struggle to spread… but those that can evade it obviously continue to do so. Even better, they don’t have to worry about the other strands of the virus crowding them out. Since the vaccine inhibits those strands, these new ones have free reign over the population.
Fast forward several thousand generations of viral replication and what are you left with? You are left with the variants that evade the vaccine. There was no world in which non-sterilizing vaccines stopped Covid in its tracks. In every single possible outcome, we end up with a virus that can evade the “vaccine.” To summarize lazily:

Pair antibody interference and viral evolution together. What does it mean? Well, it means that we have an evasive disease that doesn’t fall for the one trick pony. And you have a population of people who have become those one trick ponies and retrain themselves that one trick with every booster. What happens?
Here is a chart of booster percentage from the CDC (dark blue = higher):
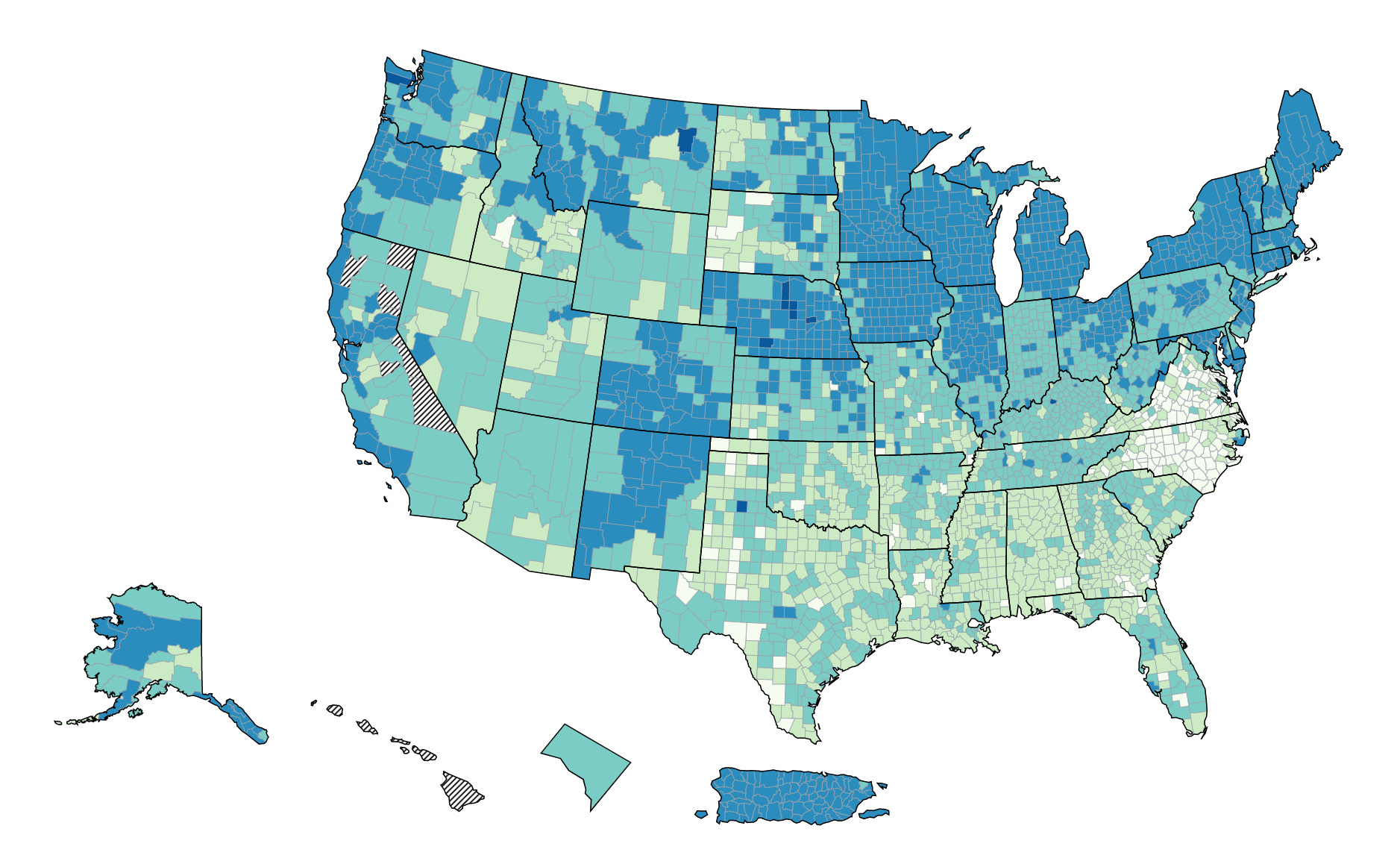
And here’s a chart of Covid community levels, also from the CDC (orange = higher):

What do you notice? There is a striking correlation between booster rates and Covid spread, particularly if you look at the Northeast and California. The correlations were even more striking a month ago, but you get the idea: places that are highly vaxxed and boosted are the areas seeing substantial infections now.
And one last thing here: it’s not actually some pandemic of the unvaccinated happening in small minorities in these states. The people who are getting sick and, unfortunately, dying are the same population as it has been: old, overweight, and otherwise at risk. No matter where you are in the country, these people were almost all vaccinated (especially in the northeast). We’ll get into that more in further updates, but this article covers evidence for that from Vermont, Israel, and the UK:
We’re going to get into this all a bit more in subsequent pieces, as well what is going on in Portugal and Australia - both highly boostered, both seeing lots of ‘roni and both sadly seeing a lot of excess death along with it.
While we cannot reach a state of conclusive proof that this is due to the “vaccines”, we will keep building up the body of circumstantial evidence until there is no other viable view.
Conclusion
There is clear evidence from analyzing antibodies that the “vaccines” being given do interfere with the body’s ability to create antibodies and train the body for one specific response to a version of the virus that is long gone. This is called Original Antigenic Sin (OAS), a well-known phenomena within virology.
What we are seeing at a macro-level with infection and death rates sadly corroborates a view that OAS is impacting the population. We see larger case spread in areas with more vaxxed and boosted populations, and increasingly the deaths we’re seeing are from populations that are also vaxxed and boosted.